Ingelief
Proud Member
what did i miss about this caligirl? who is that?
Another comment from Sprocket's blog. I highlighted interesting points. (Not necessarily ones I agree with.)
Trying not to explode from her comments (especially the notion that he would be stupid enough to drink an anesthetic, thinking it would put him to sleep. SMH.) However, she raised a couple of interesting questions and seeing as how she's in the medical field and has read the coroner's report, I'm confused as to why she still thinks 1) Michael was an addict, 2) He was in very poor health. Is the report not as vindicating as we may think? This is important to know, considering it's what Chernoff is going to pull out on Monday.
Any thoughts?
So what EXACTLY are you saying here? please go on you seem to have tons more to say.......
Well, according to the autopsy he was generally healthy. At least he didn't have any problems why he should have died. It seems to me this woman thinks he was not healthy because of the IV stand and condom catheter.
I think that's just speculation on her part. I mean, yes, they usually don't use a condom catheter and IV on healthy people, but they usually don't put healthy people under anesthesia with Propofol either.
Michael had a serious case of insomnia and he had trouble eating so he became very thin (even compared to himself) and weak. So yes, from that respect he wasn't healthy. When he was preparing for tours and was on tours unfortunately he always had these problems. Probably because of the stress and adrenaline. It's not being healthy, of course, and when you use insane methods to treat that (such as Propofol) that's not healthy either. But it's not something why he had to die. His organs were, considering his age, generally healthy - he did not have any condition which was life threatening.
I think sometimes you have to read people's "opinions" and understand they are just that...opinions. And deducing Michael was in poor shape based on IV placement is her conclusion. Doesn't make it so. Anyone that's been getting intraveneously treated over time may have some vein issues as well as ppl who are suffering from dehydration. Some ppl have naturally small veins (raises hand) to the point of having kiddie needles used on them for medical procedures.
When I see ppl drawing absolute conclusions about things which CAN have variable explanations, I generally ask myself if the person seems "open" to information contrary to their original thought. Looking at that post, I can tell you right now, she's not trying to hear otherwise. If anything, she's trying to convince others that Michael was unhealthy, in poor shape, addict, etc. With ppl like this, you just go round and round and round. I'm so done with the round and round debates now.
Maybe you can look up info about veins and what else, besides drug abuse, may cause them to be small or collapsed. The info is out there. Post that factual info to see if she validates it as a possibility contrary to her belief or if she instantly dismisses it. She might surprise you.
") and if it raises a red flag in the "addict" arena.
and if it raises a red flag in the "addict" arena.i was thinking earlier that maybe when he was younger his sleep issues werent that big of a deal because he had extra energy. this time around this is a 50yr old body and he doesnt have the same energy as he did 20yrs ago. so this time, sleep is do or die.
im not sure if this is true.. there is a rumor that he used propofol during the end of the history tour. also, like a year and a half before that, he fainted before the hbo show due to exhaustion and dehydration. does anyone think that while on tour, he may have turned to drastic measures such as propofol to get some sleep, so that episode wouldnt happen again????
Lecture 6: Introduction to IVs
We have already learned that IV stands for intravenous, or an injection that is given directly into the vein. We have a limit of 3 mL of fluid for adults when giving them subcutaneous or intramuscular injections because more than that will cause problems in the tissue surrounding the injection site, but because an IV injection goes directly into a patient's vein, the only limit on the amount of fluid that can be administered via an IV is the limit on the amount a fluid a person's body can consume without receiving more liquid than the body can absorb or excrete (which can lead to medical problems such as heart failure, high blood pressure, and excessive fluid in the lungs). The safe range of daily fluid intake will vary based on the patient's condition, size and age, as several diseases such a heart failure, kidney failure, and diabetes, for example, can require that a patient limit their daily fluid intake. Limits on a patient's fluid intake should be indicated by the doctor based on a patient's condition, but for a normal healthy adult, the normal range of total fluid intake (coming from IV fluids and/or fluids that they drink) should be 35-50 mL/kg body weight/day. For example, a 100 kg healthy adult, should get 3500-5000 mL per day of fluid, or 3.5 to 5 L. This is a lot of fluid compared to the amount that we can give using other parenteral routes of administration.
Because of this, IV administration is used when we want to give a large amount of fluid, or when we need to dilute a medication in a lot of fluid to make it the correct strength or prevent it from causing irritation. Also, because IV administration generally involves larger quantities of fluid, the medication given by IV is usually infused over a longer period of time, usually anywhere between 15 minutes and several hours. This is obviously different from subcutaneous or intramuscular injection, as these two methods involve injecting the entire medication dosage instantaneously.
Also, IV administration is faster than any other method of administation because it goes directly into the blood, so it may be used when rapid action of the drug is necessary.
Basic IV Setup
Let's take a look at a the most basic possible setup for an IV:
IVs are most often administered by bags of fluid that come premixed. The standard sizes of these bags can range from 50 mL to 1000 mL. The bag is hung from an IV pole, as we see in the picture above, and IV tubing is attached to the bottom of the bag; the IV tubing contains several important parts: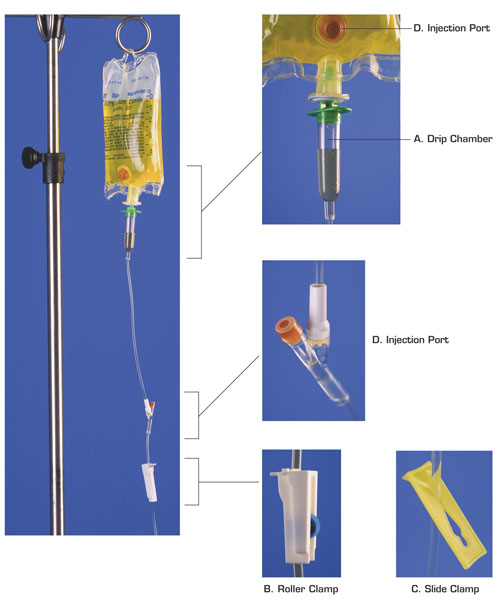
How the Height of the IV Bag Affects the Infusion Rate
- The drip chamber is located just below the IV bag; inside this chamber we can see the fluid drip down from the bag into the IV tubing. This is where we measure the speed of a manual IV setup; we look at this chamber and count the number of drops we see per minute. So, for example, if we count 25 drops over the period of 60 seconds, we would say that the IV is infusing at a rate of 25 drops per minute, or 25 gtt/min. (In reality, we may not count the number of drops in a full minute; we can, for example, count the number of drops we see over a period of 15 seconds, and then multiply that number by 4 to get the number of drops in a full minute.)
The drip chamber must always be half full. If the drip chamber is too full, we will not be able to see the drops to count them, and so we will be unable to determine the rate at which the IV is infusing. If the drip chamber is not full enough, then this will allow air to get into the IV tubing, which means that air would get into the patient's circulatory system, which could be very dangerous, blocking a blood vessel or stopping the heart.- The roller clamp is what we use to control the rate at which the IV fluid infuses. If we roll it one way, it squeezes the IV tubing more tightly, making it more narrow and therefore making the fluid flow through the tubing more slowly; if we roll it the other way, it loosens its pinching of the IV tubing, making the tubing less narrow, and allowing the IV fluid to flow through at a faster rate. So, if for example, we observe (by looking at the drip chamber and counting drops) that an IV is infusing at a rate of 50 gtt/min, but it was ordered to infuse at a rate of 30 gtt/min, we would tighten the roller clamp to slow the drip rate down until we could count only 30 drops going through the drip chamber each minute.
All roller clamps on a set of IV tubing should be closed before we attach a bag of IV fluid to the top of the tubing; this ensures that no air gets into the tubing.- Every IV medication will be ordered to infuse at a specific rate, and one of the major tasks of hosptial nurses is to set up the IV so that it infuses at this rate and to adjust the IV periodically if the rate has changed so that it remmains at the ordered rate. The rate at which an IV fluid infuses is referred to as the IV infusion rate or flow rate.
- The slide clamp is used when we want to completely stop the IV from flowing, without having to adjust the roller clamp. This is handy if we want to stop the IV for a moment, but we don't want to have to reset the flow rate by readjusting the roller clamp all over again once we start the IV up again. This works by pinching the tubing completely shut when we slide the tubing into the narrowest part of the clamp.
- The injection port is a place where medicine or fluids other than those in the current IV bag can be injected so that they will infuse into the patient's vein through the IV tubing. On the photo above we can see two ports: one on the IV bag itself and one below the drip chamber. There is also usually an injection port close to where the needle goes into the patient's vein; we'll see this below. The injection port on the actual IV bag is used if we want to mix some kind of medication with the fluid that is in the IV bag; if we inject the medication into this port and then roll the bag a little to mix the medication into the fluid in the bag, then the patient will recieve both the medication and the IV fluid at the same time. However, this can only be done when the IV fluid and the medication are allowed to be mixed. If we want to inject medication or a second kind of IV fluid directly so that it does not mix with the IV fluid that we've already attached, then we will use one of the ports that are located below the drip chamber.
IV infusion works because gravity pushes the fluid down through the IV tubing into the patient's vein. The higher the bag is hung, the greater the gravitational pressure on the IV fluid to go downward through the tubing; if the IV bag is not hung high enough, there will not be enough pressure caused by gravity to force the fluid into the vein. So, all IV bags must be hung above the patient's heart in order for there to be enough pressure for the IV fluid to infuse, and it is standard procedure to hang the IV bag at least 3 feet above an adult patient's heart to ensure there is enough pressure to keep the IV running at a constant rate.
Also, since changing the height of the IV bag changes the gravitational pressure on the fluid, a change in the bag's height over a patient's heart will change the infusion rate of the IV. If the IV bag gets higher above the patient's heart, the IV infusion rate will speed up, and if the IV bag gets lower to the patient's heart, the IV infusion rate will slow down. Because of this property, if a patient who has been lying down when the IV was set up then sits up, the IV infusion rate will slow down because the IV is now closer the to patient's heart. In fact, technically any small movement by the patient or shift in position can change the rate at which the IV is infusing. Because of this, IVs are frequently checked to make sure that they are still infusing at the correct rate; usually once an hour and after any major position change of the patient.
In addition, there are other complications of IV therapy that a nurse should watch out for. Sometimes the needle can become dislodged from the vein so that the IV fluid is no longer infusing into the vein, but rather infusing into the surrounding tissue; this is called infiltration. Some of the fluid will infuse into the tissue instead of the vein, but eventually the IV will stop because the pressure from gravity will not be enough to overcome the pressure from surrounding tissue to keep additional fluid out. Once an IV has infiltrated, a new IV must be started in a new spot on the patient's body, and the IV must be restarted at the correct rate for the given dosage. Signs that an IV has infiltrated include: pain or discomfort in the area around the IV needle, swelling in the area, the area around the needle is cool to the touch,
How the IV is attached to the patient
Here we see a picture of a common setup for inserting the IV into the patient's vein:
A cannula is a hollow needle, or more often a length of flexible plastic tubing which has been inserted into the vein using a needle; the tubing has been taped to the patient's arm to prevent it coming out when the patient moves, and a sterile dressing has been placed over the punctured place in the skin where the cannula has been inserted to prevent bacteria that commonly exist on the skin's surface from getting into the bloodstream.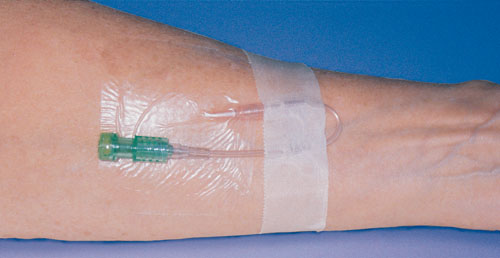
There are two different kinds of veins that can be used for the placement of the cannula; we can insert the cannula into a peripheral vein, which is any vein that is not in the torso, or we can insert the cannula into a larger more central vein in the chest.
A peripheral line is an IV that is attached to a peripheral vein, which is any vein not located in the torso. These types of IV are usually inserted into the arm or hand, although a leg or foot may be used. This is the most common type of IV.
A peripheral line may only be used for a short period of time, usually 3 days, because if it is used for longer periods of time, bacteria that are normally present on the skin can travel into the blood or the tissue surrounding the injection site and cause infection. So, if a peripherial line is needed for more than 3 days, it is standard procedure to move the injection site to a new location every 3 days to prevent infection. Both the pictures above and below show peripheral lines.
A central line is an IV that is attached to a vein in the chest. Usually the cannula is inserted through the chest wall or a neck vein, but it is also possible to insert the cannula into a peripheral vein an then to move the tip of the cannula slowly upward until it is in a central vein.
Central veins are much larger than peripheral veins, so when a central line is used and the cannula is inserted through the chest or neck the tubing can be wider and so multiple smaller tubes can be inserted through the larger one to deliver several IV medications at once that are not allowed to mixed. Also, a central line goes into a vein that carries blood directly to the heart, so medication given this way is distributed more quickly throughout the body. Medicines that are particularly harsh or in a high concentration are also more likely to irritate a peripheral vein, such as chemotherapy drugs and some kins of liquid nutrition, can be given in a central line when they are too irritating to be administered via a peripheral vein.
However, a central IV line is also more likely to cause bleeding and the risks of infection are much higher because the contents of the line go directly to the heart, so any bacteria that get into the line are quickly spread throughout the body; also, the risks of getting air in the line that could block veins or stop the heart are higher with a central line since it is wider and therfore allows for larger amounts of air to enter (the more air that enters the bloodstream, the greater the danger that a vein will be blocked or the heart will stop).
Here we can see a picture of a patient with a central line:
Continuous versus Intermittent IV Infusion
Sometimes an IV medication or fluid is given continuously, or all the time. But sometimes we may want to administer an IV fluid and/or medication to a patient only at specific times; this is called an intermittent IV infusion. A patient may receive only continuous IV fluids/medication, or only intermittent IV fluids/medication or a mixture of both.
A patient who is to recieve a continuous IV has the IV setup connected to them all the time, but for a patient who should receive only intermittent IVs, we can't leave them permanently attached to an IV setup. What we do instead is insert a cannula like the one in the picture below to the patient, which allows us to connect an IV only when the patient is actually receiving an infusion and to disconnect it in between doses:
This is a length of IV tubing with an injection port attached to one end; this special injection port is called an infusion port adapter, although it is also usually referred to as a heplock or a saline lock/port, because in an intermittent IV setup, the patient is not getting a constant flow of fluid through the cannula, so it can become blocked by clotted blood and therefore must be flushed periodically in order to clear it out; heparin (in a concentration of 100 U/mL), a drug which prevents blood from clotting, and saline, or salt water, are the two fluids that are used for this flush, which involves an injection of approximately 1-2 mL of either of these fluids every 6 to 8 hours.
Secondary IV or IV Piggyback
If a patient is receiving continuous IV fluids and/or medication and in addition must receive a second kind of intermittent infusion, or if a patients current IV infusion must be interrupted in order to administer a second IV medication or fluid that is more pressing, then we will need to hang a secondary IV for the patient. A secondary IV, also know as IV Piggyback, and abbreviated IVPB, is a second IV medication or fluid that is hung alongside the first and which is attached to the first set of IV tubing through one of the injection ports that is below the drip chamber of the primary IV (if we were to connect it through the injection port inside the primary IV bag, the contents of the primary and secondary IVs would mix and infuse at the same time, which is not what we want).
A secondary IV is usually used for medications and usually contains a smaller volume than the primary IV; secondary IV bags are usually 50-250 mL, while the most frequently used primary IV bags are 500 or 1000 mL. Generally a secondary IV is an intermittent medication that we want to interrupt the administration of the primary IV medication or fluids given continuously, and then we want the primary IV to resume infusing after the secondary IV has finished. Because we want the secondary IV to infuse first, we must hang the secondary IV higher than the primary IV. To do this we attach an extender to the top of the primary IV bag to lower it so that the top of the primary IV bag is below the bottom of the secondary IV bag (see the picture below).
The picture below shows a secondary IV set up to the left and the primary IV hung to the right:
Notice that in this picture, the secondary IV bag is above the primary IV bag; this means that the pressure on the secondary IV bag will be greater than the pressure on the primary IV bag, and so this pressure will push it down into the tubing and prevent any of the fluid from the primary IV from entering the tubing until the secondary IV has emptied. Then, once the secondary IV has finished infusing, the primary IV will be able to go down into the tubing again, and the infusion of the primary IV will resume. Notice also that each IV bag has its own drip chamber (and although you cannot see it in this picture, each IV bag has its own clamps as well) so that we can measure and control the flow rate to each bag separately; this is because the primary and secondary IVs will probably not be ordered to infuse at the same rate and we will need to set the flow rate on the secondary IV separately from the flow rate of the primary IV.
IV Push or Bolus
Sometimes we may want to give a medication by IV, maybe because it is a larger volume than 3 mL or because it will be absorbed better that way, but we are not giving a large enough volume or a strong enough concentration that we need to give the medication over an extended period of time; we may want to just give the medication in one immediate shot, just like when we give an IM or subQ injection. In this case, we can simply inject the medication into one of the injection ports on an IV line; giving a medication all at once by inserting a syringe into one of the injection ports is called IV push or bolus.
We can give an IV bolus to a patient who already has a continuous IV setup or we can inject the IV push directly into a heplock which has been set up for intermittent IV administration. Below we see a photo of a nurse giving a patient an IV bolus by injecting it into the injection port closest to the cannula, interrupting a continuous IV that is already in place:

respect77;3181265 said:I think so, yes. I think he always had a problem with sleeping (even when he was not on tour), but when he was on tour he HAD to sleep somehow to be able to perform the next day. And unfortunately he couldn't find any other solution.
I don't know if he ever tried to ask professional help for his sleep problems. And by professional help I don't mean shady doctors who would give him Propofol, but somebody who was an expert of insomnia treatment.
Quick question...
If Michael had injected himself, would he be coughing or would he be out of it straight away?
No no, not with the judge. There are lawyers reviewing the case in the overflow room and Erin's next door neighbor is there and works for a lawyer firm. His actions warrant a higher charge which is blatantly obvious she said. But this whole prelim scenario is very "old school" she said. It shows the defense what its up against which makes no sense for the state in this instance so why this is happening is insane she said.
According to the pros, even going this route, the prelim should have been stopped and a decision made whether to proceed to trial with IM as the charge or up the charge and proceed or refile and start again with a new charge. (Which one of these will ultimately happen is unknown but I'd PERSONALLY assume this is being dragged out to show the DA the charges need to be upped.)
Michael was afraid of needles so he would have never ever tried that.
Michael was afraid of needles so he would have never ever tried that.
True, was afraid of needles and wasn't exactly an impulsive person to do that to himself.
Is it true that Murray may be offered a plea bargain after the preliminary hearing? I just heard some talk about it yesterday. If it is true, what will happen if he pleads guilty? :scratch:
Is it true that Murray may be offered a plea bargain after the preliminary hearing? I just heard some talk about it yesterday. If it is true, what will happen if he pleads guilty? :scratch:
there was no diprivan found in the iv bag the claim is he injected into himself.On top of that, he would have had to place more bottles of propofol in the IV bag while under the drugs Murray had already given him...
theres always a chance but i doubt as there isnt really anything to plea down to if he pleads guilty to something then no trial just sentencing
There are so many things that are questionable about this case. But one of the most glaring for me is the fact that we're going into two years since this happened and they still can't nail down a solid timeline. Murray's lawyers say he never gave the police an official timeline. Well, why not? All this time that's gone by and he still hasn't done that? That should have been done the first time the police interviewed him. This is ridiculous.
he gave a very detailed timeline when he was interviewed by the police a couple of days after the 25th including a timline of when he gave all the drugs. he just changed it later when he realised it made him look even more guilty
ray: ray:I assumed that IF Michael was using an IV for sleep, that he would want any marks from the needle to be hidden under his clothes. He had children that he would want to protect from seeing that. I read somewhere that the amount of propofol used by Murray from the orders, would not have been enough for 6 weeks - more like 1 week. I hope we find out if this is true or not.
Ortega said, back then, that he talked with Mike around 3am about concerts. That means if Mike called, he was awake at 3 am couple of weeks or week before, June 25 ( cannot remember well what Ortega said )
So Mike was not under Propofol under those nights. And if he got a morning routine and went through it those specific mornings, we can assume that he was not under Propofol those nights.
Also, observing Murray 'ways' of applying and monitoring anesthesia
I wonder if Mike knew about Propofol at all....
( some doctors might said Mike begged for it, but heck all world knew already about propofol and maybe they just wanted to look good in the eyes of the world 'look some good doctors that said No to Michael Jackson nuttiness, some heroes here )
I know it's just me assuming, but if Murray apply this type of anesthesia on Mike more than once, how Mike survived?? :mello:
I mean why be reckless one night and assume other nights he was good doctor? ( unless Nurray was drunk or drugged that specific night, and not in the rest )
How many times can pure luck work with this stupid way of anesthesia? Is there any LUCK at all with this disaster anesthesia??